It is thus one of a constellation of associated lipid accumulation disorders connected with hyperinsulinaemia, the others including atherosclerosis, NAFLD, obesity. That these conditions are linked in some way was recognised as early as the 1880s by the great German physiologist Wilhelm Ebstein, the father of the modern LCHF diet.[2]
In the recent saturated fat and disease meta-analysis by de Souza et al, higher intake of ruminant trans-palmitoleic acid, a marker of dairy fat consumption, was inversely associated with type 2 diabetes (0.58, 0.46 to 0.74).[3] This is consistent with many studies of serum biomarkers of dairy fat consumption, also including odd-chain saturated fatty acids.
The recent results from Malmö, the third largest city in Sweden, give more detail about these correlations. The Malmö Diet and Cancer cohort was studied using a 7-day food diary and a 1 hour interview as well as an FFQ. This makes the results more reliable than other epidemiological diet studies, which normally use only the FFQ. In Malmö, greater consumption of dairy fat (including butter) had a protective association with T2D. The association was strongest for shorter-chain fatty acids (from 4:0, butyrate, to 14:0, myristic acid) and there was also a protective effect of a higher ALA/LA ratio.[4]
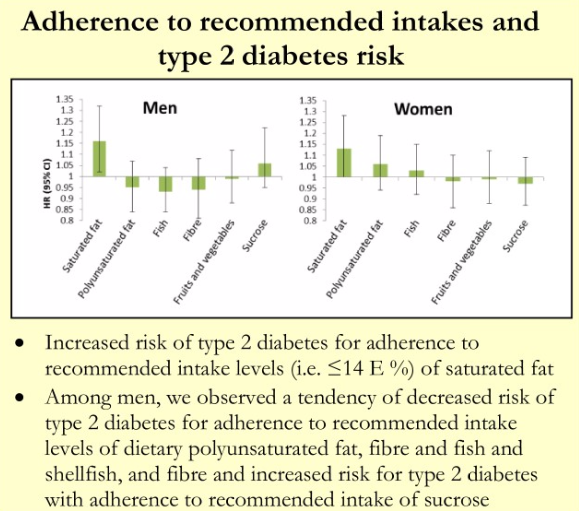
In a separate analysis of the Malmö cohort, it was found that adherence to dietary recommendations to limit saturated fat to 14% or less of energy was associated with a 15% increased risk of T2D in men and a slightly smaller increase in women. There was a small association in men between adherence to recommendations to limit added sucrose and T2D.[5] (I see a future paper here titled “food sources of sucrose may clarify the inconsistent role of dietary sucrose intake for incidence of type 2 diabetes”. After all, chocolate consumption has beneficial associations not seen with sugar sweetened beverages.)

Is there some simple, mechanical explanation that
begins to explain the relationship? If T2D is the result of excess lipid
storage, are some lipids easier to store than others? NAFLD research suggests
that short- to medium-chain fatty acids are not easily stored. Wistar rats fed
coconut oil under NAFLD-generating conditions ate an incredible 143% extra
calories across the board with no increase in hepatic lipid accumulation, while
butter-fed rats managed an extra 30%.[6]
A team led by George Bray looked at rates of fatty acid oxidation in humans, and made two findings - 1) the shorter the chain length of a saturated fat, the faster the rate of oxidation, 2) the more double bonds in an unsaturated fat, the faster the rate of oxidation. Thus, lauric acid (12:0) was oxidised at a much higher rate than stearate (18:0), and ALA (18:3) was oxidised at a faster rate than LA (18:2).[7]
The faster a fatty acid is oxidised the harder it is to store; this phenomenon discourages lipid accumulation, with benefits to the risk of lipid accumulation disorders.
A team led by George Bray looked at rates of fatty acid oxidation in humans, and made two findings - 1) the shorter the chain length of a saturated fat, the faster the rate of oxidation, 2) the more double bonds in an unsaturated fat, the faster the rate of oxidation. Thus, lauric acid (12:0) was oxidised at a much higher rate than stearate (18:0), and ALA (18:3) was oxidised at a faster rate than LA (18:2).[7]
The faster a fatty acid is oxidised the harder it is to store; this phenomenon discourages lipid accumulation, with benefits to the risk of lipid accumulation disorders.

A second consideration is that fat displaces carbohydrate in the diet, and carbohydrate is the nutrient that, by inducing insulin secretion, increases lipid synthesis and lipid conservation, something that (without the insulin bit) Wilhelm Ebstein understood in the 1880s. Levels of serum triglycerides are directly associated with %E from carbohydrate, and this triglyceride component is the source of pancreatic fat in the model of Professor Roy Taylor.[1]
A third consideration is that saturated fats are resistant to peroxidation and oxidative stress plays a role in promoting beta-cell failure. Saturated fats are protective against beta-cell failure in the alloxan-treated rat.
http://caloriesproper.com/diet-diabetes-and-death-oh-my/
References
[1] Taylor, R. Type 2 Diabetes. Etiology and reversibility. Diabetes Care April 2013;36(4): 1047-1055
[2] Wilhelm Ebstein. Corpulence and its treatment on physiological principles. 1882. https://archive.org/details/corpulenceitstre00ebst
[3] de Souza, RJ, Mente, A, Maroleanu, A, Cozma, AI, Ha, V, Kishibe,T, et al. Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: systematic review and meta-analysis of observational studies. BMJ 2015;351:h3978
[1] Taylor, R. Type 2 Diabetes. Etiology and reversibility. Diabetes Care April 2013;36(4): 1047-1055
[2] Wilhelm Ebstein. Corpulence and its treatment on physiological principles. 1882. https://archive.org/details/corpulenceitstre00ebst
[3] de Souza, RJ, Mente, A, Maroleanu, A, Cozma, AI, Ha, V, Kishibe,T, et al. Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: systematic review and meta-analysis of observational studies. BMJ 2015;351:h3978
[4] Ericson, U, Hellstrand, S, Brunkwall, L, Schulz,
C-A, Sonestedt, E, Wallström, P, et al. Food sources of fat may clarify the
inconsistent role of dietary fat intake for incidence of type 2 diabetes. AJCN
2015;114.103010v1
[5] Sonestedt, E et al. A high diet quality based on dietary recommendations does not reduce the incidence of type 2 diabetes in the Malmo Diet and Cancer cohort. EADS2015 ePoster #322 http://www.easdvirtualmeeting.org/resources/a-high-diet-quality-based-on-dietary-recommendations-does-not-reduce-the-incidence-of-type-2-diabetes-in-the-malmo-diet-and-cancer-cohort--3
[6] Romestaing, C, Piquet, MA, Bedu, E, Rouleau, V, Dautresme, M, Hourmand-Ollivier, I et al. Long term highly saturated fat diet does not induce NASH in Wistar rats. Nutr Metab (Lond). 2007; 4: 4
[7] DeLany, JP, Windhauser, MW, Champagne, CM, Bray, GA. Differential oxidation of individual dietary fatty acids in humans. Am J Clin Nutr October 2000;72(4): 905-911
[5] Sonestedt, E et al. A high diet quality based on dietary recommendations does not reduce the incidence of type 2 diabetes in the Malmo Diet and Cancer cohort. EADS2015 ePoster #322 http://www.easdvirtualmeeting.org/resources/a-high-diet-quality-based-on-dietary-recommendations-does-not-reduce-the-incidence-of-type-2-diabetes-in-the-malmo-diet-and-cancer-cohort--3
[6] Romestaing, C, Piquet, MA, Bedu, E, Rouleau, V, Dautresme, M, Hourmand-Ollivier, I et al. Long term highly saturated fat diet does not induce NASH in Wistar rats. Nutr Metab (Lond). 2007; 4: 4
[7] DeLany, JP, Windhauser, MW, Champagne, CM, Bray, GA. Differential oxidation of individual dietary fatty acids in humans. Am J Clin Nutr October 2000;72(4): 905-911
9 comments:
Some extra thoughts on this - of course there wasn't much coconut oil in Malmo and epidemiological data on coconut oil and diabetes is hard to some by. However, there is a bit of data about metabolic syndrome from the Phillippines, where coconut oil is a common cooking fat, e.g.
Kuzawa CW, Adair LS, Avila JL, Cadungog JH, Le NA. Atherogenic lipid profiles in Filipino adolescents with low body mass index and low dietary fat intake. Am J Hum Biol. 2003 Sep-Oct;15(5):688-96. http://www.ncbi.nlm.nih.gov/pubmed/12953181
Feranil,AB, Duazo, PL, Kuzawa, CW, Adair, LS. Coconut oil predicts a beneficial lipid profile in pre-menopausal women in the Philippines. Asia Pac J Clin Nutr. 2011; 20(2): 190–195 http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3146349/
Is there an insulinogenic effect of Lauric acid, and should this matter? There is here:
Garfinkel M, Lee S, Opara EC, Akwari OE. Insulinotropic potency of lauric acid: a metabolic rationale for medium chain fatty acids (MCF) in TPN formulation. J Surg Res. 1992 Apr;52(4):328-33 http://www.ncbi.nlm.nih.gov/pubmed/1593871
Why should this be? If your liver is going to start generating ketones in a non-hormonal way because you've eaten MC fats, you'll be needing less glucose in the blood. A squirt of insulin to inhibit glucagon and lower BG before these ketone bodies appear thus makes sense.
The response to LA in that paper may have a different rationale - LA is preferentially converted to cholesterol (22%), palmitate and other lipids and this lipogenesis, which seems to be a safety feature, perhaps requires insulin. Maybe.
The Malmo study was designed as a Cancer study. Its data collection methods seem to have been exemplary and to have taken on board criticisms of the FFQ approach. One of the papers I cited in this post even used a model excluding people who changed their diet during the follow-up. With that in mind, what did they learn about cancer?
Wirfält E, Mattisson I, Gullberg B, Olsson H, Berglund G. Fat from different foods show diverging relations with breast cancer risk in postmenopausal women. Nutr Cancer. 2005;53(2):135-43. http://www.ncbi.nlm.nih.gov/pubmed/16573374
Fat from fermented milk products was negatively associated with breast cancer risk (trend, P = 0.003). The highest quartiles of vegetable oil-based dietary fats (odds ratio, OR = 1.74; confidence interval, CI = 1.12-2.72) and dried soup powders (OR = 1.59; CI = 1.04-2.43) showed positive associations. Dietary fiber did not influence associations.
Dried soup powders are cancer promoters? Maggi, Cup a Soup and all that crap? This does not surprise me one bit. Also, in this case control study, controls ate more meat and sausage than cases.
.
Correction, I misread that table, cases and controls ate much the same amounts of meat.
Interesting++ George, the Taylor paper is good too. Maybe you can find more data if you broaden out the search to palm oil or palm kernel oil. PKO is 48% myristic ~16% lauric and ~15% oleic with a little palmitic.
C.
nice analysis George.
"Dietary fiber did not influence associations." ==> consistent with past evidence AFAIK.
"If your liver is going to start generating ketones in a non-hormonal way because you've eaten MC fats, you'll be needing less glucose in the blood. A squirt of insulin to inhibit glucagon and lower BG before these ketone bodies appear thus makes sense." ==> makes sense to me to. Hadn't thought of it like that though. Should a prediction from this theory then be that glucagon in a high MCT (say coconut oil) keto diet would be lower overall & pulsate differently than it otherwise would in a very low MCT (say butter) keto diet context? if that makes sense...
Rats infused with MCT fats have higher insulin, but less weight gain, than rats infused with LCT fats.
http://jn.nutrition.org/content/122/7/1483.long
More fro Malmo - Unfortunately this one used "food pattern" analysis which is pretty useless.
http://aje.oxfordjournals.org/content/154/12/1150.full
The study demonstrated relations, independent of specific nutrients, between food patterns and hyperglycemia and central obesity in men and hyperinsulinemia in women. Food patterns dominated by fiber bread provided favorable effects, while food patterns high in refined bread or in cheese, cake, and alcoholic beverages contributed adverse effects. In women, food patterns dominated by milk-fat-based spread showed protective relations with hyperinsulinemia.
With the exception of cancer mortality for women in the highest quartile of relative fat intake, individuals receiving more than 30% of their total daily energy from fat did not have increased mortality. Men in the fourth quartile of total fat intake, receiving almost 50% of their total energy intake from fat, had the lowest cardiovascular mortality. Receiving more than 10% of total energy intake from saturated fat did not have a significant effect on all-cause, cardiovascular or cancer mortality for men or women. Beneficial effects of relatively high intakes of unsaturated fats were not uniform, and having a high index of unsaturated fat compared with saturated fat intake did not have any detectable effect on mortality.
http://onlinelibrary.wiley.com/doi/10.1111/j.1365-2796.2005.01520.x/full
Medium-chain fatty acids: Functional lipids for the prevention and treatment of the metabolic syndrome. Koji Nagao, , Teruyoshi Yanagita. Pharmacological Research
Volume 61, Issue 3, March 2010, Pages 208–212
Abstract
Metabolic syndrome is a cluster of metabolic disorders, such as abdominal obesity, dyslipidemia, hypertension and impaired fasting glucose, that contribute to increased cardiovascular morbidity and mortality. Although the pathogenesis of metabolic syndrome is complicated and the precise mechanisms have not been elucidated, dietary lipids have been recognized as contributory factors in the development and the prevention of cardiovascular risk clustering. This review explores the physiological functions and molecular actions of medium-chain fatty acids (MCFAs) and medium-chain triglycerides (MCTs) in the development of metabolic syndrome. Experimental studies demonstrate that dietary MCFAs/MCTs suppress fat deposition through enhanced thermogenesis and fat oxidation in animal and human subjects. Additionally, several reports suggest that MCFAs/MCTs offer the therapeutic advantage of preserving insulin sensitivity in animal models and patients with type 2 diabetes.
J Nutr Sci Vitaminol (Tokyo). 2011;57(2):138-43.
Dietary medium-chain triglycerides attenuate hepatic lipid deposition in growing rats with protein malnutrition.
Kuwahata M1, Kubota H, Amano S, Yokoyama M, Shimamura Y, Ito S, Ogawa A, Kobayashi Y, Miyamoto K, Kido Y.
Abstract
The objective of this study was to investigate the effects of dietary medium-chain triglycerides (MCT) on hepatic lipid accumulation in growing rats with protein malnutrition. Weaning rats were fed either a low-protein diet (3%, LP) or control protein diet (20%, CP), in combination with or without MCT. The four groups were as follows: CP-MCT, CP+MCT, LP-MCT, and LP+MCT. Rats in the CP-MCT, CP+MCT and LP+MCT groups were pair-fed their respective diets based on the amount of diet consumed by the LP-MCT group. Rats were fed each experimental diet for 30 d. Four weeks later, the respiratory quotient was higher in the LP-MCT group than those in the other groups during the fasting period. Hepatic triglyceride content increased in the LP groups compared with the CP groups.
Hepatic triglyceride content in the LP+MCT group, however, was significantly decreased compared with that in the LP-MCT group. Levels of carnitine palmitoyltransferase (CPT) 1a mRNA and CPT2 mRNA were significantly decreased in the livers of the LP-MCT group, as compared with corresponding mRNA levels of the other groups. These results suggest that ingestion of a low-protein diet caused fatty liver in growing rats. However, when rats were fed the low-protein diet with MCT, hepatic triglyceride deposition was attenuated, and mRNA levels encoding CPT1a and CPT2 were preserved at the levels of rats fed control protein diets.
Post a Comment