(Music: Charlie Parker Live at Storyville, 1953)
Coeliac and non-coeliac gluten sensitivity, conditions which can cause (apart from the classic syndrome) cirrhosis of the liver independent of viruses or alcohol, are hard to treat by simple removal of gluten grains, because gliadin sensitivity creates cross-sensitivity to peptides found in other foods.
(Hat-tip to Suppversity for posting about this).
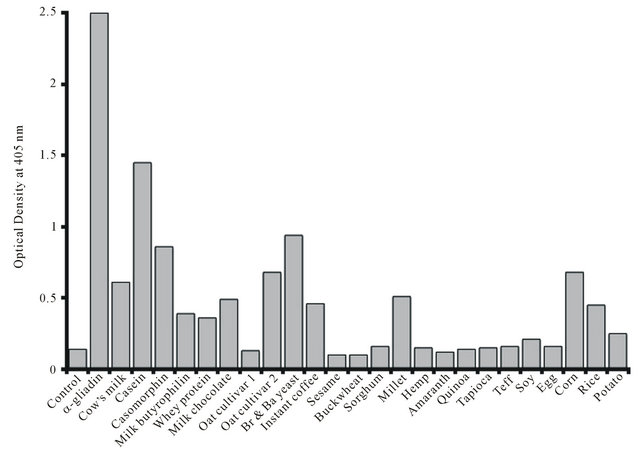
Gliadin (Wheat), Casein (Milk), Secalin (Rye), Avenin (Oat), Kafirin (Sorghum), and Zein (Corn) peptides are prolamines (peptides with Pro-Pro bonds). But why does instant coffee feature at all? Well, coffee is a seed, but it doesn't appear to be a source of prolamines.
All of these cross-sensitivity prolamine allergens are also active at endorphin receptor sites; they are what is called exorphins. Wheat and milk can be addictive to persons who should be avoiding them, another reason coeliac is difficult to diagnose and treat. And roasted coffee beans also contain a compound which has endorphin receptor activity - except that it is an endorphin antagonist, and not a prolamine but a lactone formed from one of coffee's antioxidants.
There is no record of a link between coeliac disease and endorphins (at least, none that the cursory Google search that easily supplies all my other evidential links has uncovered), beyond the helpfulness of LDN (low dose Naltrexone) in CD recovery.
However, opioids (at least, the pharmaceutical ones) have two modes of action, one via the endorphin system, one via the immune system and TRL4 activity. Naltrexone is both an opioid antagonist and a TLR4 antagonist; and TLR4 is implicated in coeliac disease via non-gluten components of wheat, trypsin inhibitors.
(At about this point, the trail went cold. It would have been nice to link exorphins and TLR4, I had even dreamed about TLR4 antagonism and the benefits of coffee drinking, but it was not to be...)
Edit: here is a link between coffee and TLR4 inhibition, it's not about the exorphin, but there's hope for me yet.
 |
| Enlarged picture here |
Coeliac and non-coeliac gluten sensitivity may be associated with Hepatitis C, and anecdotally a great many people with the virus find their health improves when avoiding the cross-reactive foods. Both coeliac disease (OR 3.1) and chronic HCV infection (OR 2-4) are associated with an increased rate of non-Hodgkin's lymphoma, and the autoimmune conditions commonly associated with coeliac are virtually identical to the extra-hepatic HCV syndrome. As an intracellular virus, HCV triggers the production of interferons, and interferon-alpha has a causitive role in coeliac. Coeliac disease has been triggered by INF-alpha treatment for HCV. However, gluten sensitivities are hard to diagnose and exist on a spectrum, with a significant proportion of people having some potential for sensitivity, and gluten sensitivity diseases may take time to develop. On average, cases of coeliac disease take 13 years to diagnose. This is plenty of time for someone to develop serious health problems or indeed die, without the involvement of gluten sensitivity being noticed.
(I have never been a fan of Interferon treatment for HCV; in my experience people who have avoided Interferon and treated themselves with diet and supplements tend to stay healthier overall than people who have done interferon but failed to respond to it. Indeed, I know people with chronic hepatitis C who stay healthy with no effort at self-treatment whatsoever. So far, the people I have known with HCV who have died of liver disease or needed transplants, other than alcoholics, are people who have taken Interferon but failed to clear the virus. People who do respond to Interferon can certainly improve, but this means that doctors prescribing Interferon need to be selective about who they offer it to. If it is prescribed to someone with no symptoms, or a low possibility of clearance, or a high risk of side effects on the basis that this is better than doing nothing, this is unlikely to be the case. Thankfully this question is becoming moot with the arrival of interferon-free treatments with a high rate of efficacy and minimal side-effects. Here is a grueling account of post-interferon problems.)
I think it entirely plausible that the post-treatment effects some people experience from Interferon therapy for HCV are mediated by the induction of sensitivity to wheat, milk, yeast, corn and other foods, and that the extra-hepatic and autoimmune syndromes of chronic hepatitis C have the same cause. This could include a wide variety of auto-immune conditions, not just gut disorders.
On the other hand, I am not in favour of eliminating so many foods from the diet that nutrition is compromised. Removing the main offenders - grains, legumes (also a source of trypsin inhibitors), yeast (bread and beer are the main sources of yeast), and milk (some dairy products low in casein, such as butter, may be OK), supplementing vitamin D and probiotics, and eating nutrient-dense foods mainly of animal origin for a while seems to be the best way to both heal the gut and reduce autoimmunity.
Another problem with grains, and with milk in people who are lactose intolerant, is SIBO, or an excess of bacteria in the small intestine. This is associated with progression of NASH and cirrhosis, and also with Vitamin B12 deficiency. It's a good fibre/bad fibre situation, with good fibres being those that ferment in the colon (large intestine).
Micheal Eades has just blogged about SIBO in the context of GERD, a common cause of eosophagitis (acid reflux, sore throat, difficulty swallowing, increased cancer risk).
Reading first the introduction to a vitamin primer, and then Protein Power, by Drs Michael and Mary Dan Eades first awakened me to the possibilities of low-carb, high fat diets for the treatment of inflammation and autoimmune disease. I'd like to thank the Drs Eades for writing books that became popular enough to become ubiquitous (and thus arrive at the Op Shops I get my books from) while remaining readable.
Here's one of my favourite NASH papers, just an abstract from a poster presentation at a conference - but how on earth does anyone get an omega 3:6 ratio of 1:144? Note that no-one here had 3:6 in or near the adaptive range of 1:1 - 1:5.
Methods: 15 patients (10 female) underwent analysis of erythrocyte lipid composition using capillary gas chromatography (Metametrix, Duluth, GA) to determine the AA:EPA ratio. The mean age was 50 ± 13 years all with liver biopsy NAS score ≥ 5 and a range of non-cirrhotic fibrosis stages of stage 1 (n = 6), stage 2 (n = 5) and stage 3 (n = 4).
Results: The mean AA:EPA was 65 ± 34 reflecting a relative excess of n-6 PUFA overall. However, a broad range was noted from 15 to 144 AA:EPA. Dividing the group into quintiles of the reference range, 9 of the patients fell into the highest (5th) quintile (AA:EPA = 84 ± 30) compared to the remaining 6 patients (AA:EPA = 36 ± 16, p = 0.001). There was no statistically significant difference in the histological stage between these groups (fibrosis score = 2 ± 0.9 versus 1.7 ± 0.8) although the higher AA:EPA group was significantly older (55±12 versus 39±12, p=0.01).
Conclusion: There is heterogeneity of AA:EPA in non-cirrhotic NASH patients and an age-related increase in n-6 to n-3 PUFA evident in the AA:EPA ratio of erythrocyte lipids. Further work is needed to understand if this reflects dietary differences and how this might influence response to omega-3 fatty acid therapy.
I think it entirely plausible that the post-treatment effects some people experience from Interferon therapy for HCV are mediated by the induction of sensitivity to wheat, milk, yeast, corn and other foods, and that the extra-hepatic and autoimmune syndromes of chronic hepatitis C have the same cause. This could include a wide variety of auto-immune conditions, not just gut disorders.
On the other hand, I am not in favour of eliminating so many foods from the diet that nutrition is compromised. Removing the main offenders - grains, legumes (also a source of trypsin inhibitors), yeast (bread and beer are the main sources of yeast), and milk (some dairy products low in casein, such as butter, may be OK), supplementing vitamin D and probiotics, and eating nutrient-dense foods mainly of animal origin for a while seems to be the best way to both heal the gut and reduce autoimmunity.
Another problem with grains, and with milk in people who are lactose intolerant, is SIBO, or an excess of bacteria in the small intestine. This is associated with progression of NASH and cirrhosis, and also with Vitamin B12 deficiency. It's a good fibre/bad fibre situation, with good fibres being those that ferment in the colon (large intestine).
Micheal Eades has just blogged about SIBO in the context of GERD, a common cause of eosophagitis (acid reflux, sore throat, difficulty swallowing, increased cancer risk).
Reading first the introduction to a vitamin primer, and then Protein Power, by Drs Michael and Mary Dan Eades first awakened me to the possibilities of low-carb, high fat diets for the treatment of inflammation and autoimmune disease. I'd like to thank the Drs Eades for writing books that became popular enough to become ubiquitous (and thus arrive at the Op Shops I get my books from) while remaining readable.
Here's one of my favourite NASH papers, just an abstract from a poster presentation at a conference - but how on earth does anyone get an omega 3:6 ratio of 1:144? Note that no-one here had 3:6 in or near the adaptive range of 1:1 - 1:5.
POLYUNSATURATED FATTY ACID COMPOSITION IN ERYTHROCYTE LIPID MEMBRANES IN NASH: UNEXPECTED HETEROGENEITY IN THE N6-N3 RATIO
S. Caldwell*, C. Argo, A. Al-Osaimi, N. Shah, H. Lothamer, C. Harmon, J. Rodriguez
University of Virginia, Charlottesville, VA, USA. *shc5c@virginia.edu
University of Virginia, Charlottesville, VA, USA. *shc5c@virginia.edu
Introduction and aim: Essential dietary polyunsaturated fatty acids (PUFA) include omega-6 (n-6) linoleic acid (18:2) which is metabolized to arachidonic acid (AA) and omega-3 (n-3) linolenic acid (18:3) which is metabolized to eicosapentanoic acid (EPA). Imbalance in secondary eicosanoids and prostaglandin metabolites of n-6 and n-3 PUFA are implicated in disorders related to the metabolic syndrome. Skeletal muscle PUFA influences systemic insulin sensitivity (Borkman 1993) and diets rich in omega-3 fatty acids are associated with diminished histological injury in NASH (Musso 2003). Erythrocyte membrane lipids reflect dietary intake of essential fatty acid over preceding months. We measured erythrocyte n-6:n-3 ratio in a cohort of patients as part of a larger study of omega-3 fatty acid therapy of NASH.
Methods: 15 patients (10 female) underwent analysis of erythrocyte lipid composition using capillary gas chromatography (Metametrix, Duluth, GA) to determine the AA:EPA ratio. The mean age was 50 ± 13 years all with liver biopsy NAS score ≥ 5 and a range of non-cirrhotic fibrosis stages of stage 1 (n = 6), stage 2 (n = 5) and stage 3 (n = 4).
Results: The mean AA:EPA was 65 ± 34 reflecting a relative excess of n-6 PUFA overall. However, a broad range was noted from 15 to 144 AA:EPA. Dividing the group into quintiles of the reference range, 9 of the patients fell into the highest (5th) quintile (AA:EPA = 84 ± 30) compared to the remaining 6 patients (AA:EPA = 36 ± 16, p = 0.001). There was no statistically significant difference in the histological stage between these groups (fibrosis score = 2 ± 0.9 versus 1.7 ± 0.8) although the higher AA:EPA group was significantly older (55±12 versus 39±12, p=0.01).
Conclusion: There is heterogeneity of AA:EPA in non-cirrhotic NASH patients and an age-related increase in n-6 to n-3 PUFA evident in the AA:EPA ratio of erythrocyte lipids. Further work is needed to understand if this reflects dietary differences and how this might influence response to omega-3 fatty acid therapy.
Here is a discussion of changing omega 3:6 in the US food supply: "The ratio of total n−6 to n−3 was 5.4 in 1909 and 9.6 in 1999". Average intake of omega 6 has always been sufficient but has become excessive, intake of omega 3 has always been inadequate.
15 comments:
I like your post. It is very interesting. I am also very health conscious.
Regards,
Kopi Luwak
Actually, if you wanted to maximise your intake of chlorogenic acid from coffee, and minimize you exposure to the cross-reactive lactone (or acrylamide), then green-er coffee would be just the thing.
You might not be able to afford the help of a stress-free palm civet, but products like this are cheap and palatable.
http://fresh.co.nz/love-coffee-and-tea-try-green-tea-coffee/
Nestle of course are the devil incarnate, but there is bound to be a FairTrade version somewhere.
I would only add that this is seen in other postviral fatigue/malaise situations also, not just following HCV infection. What all these situations appear to have in common is autoimmunity and compromised intestinal integrity.
Yes, that's right. It's part of the etiology of CFS/ME post-glandular fever (etc). I've also seen a study of gluten sensitivity during viral infections that resolved after the virus cleared (but haven't been able find it again).
It's a truism that most colds and flus, also ear infections, create sensitivity to milk and resolve much quicker if milk is withdrawn from the diet.
People who tolerate these foods do so because their immune system keeps quiet about the antigens in them. When you are fighting an infection, it's harder for the immune system to keep quiet.
It looks like the interferon therapy is another case of too unhealthy treatment for a health problem. Guys, choose your poison.
I read all you write about a treatment for HepC because I have a relative with a such condition (a-symptomatic so far).I guess, the pleasure of the reading would be the only result. It is , unfortunately, a very small chance she would opt for a LCHF diet.
I meet people who did well on interferon and are better now; but it's definitely a risk, and one that isn't appreciated, or is only being appreciated now, because they have new drugs to sell.
Fortunately the new drugs do appear to be as good and as safe as anyone could reasonably expect.
If she has no symptoms, I'd wait till these new drugs are perfected.
Great, George. And thanks for the link to the green nescaf. On a totally unrelated note, I feel compelled to comment on the Minoan (Mycenaean) 'Mother Goddess' image on your page (hint: not a mother goddess ;) ). The idol is one of 14 unprovenienced works from Evans' 4th campaign at Knossos. The figurines - conspicuously characteristic of Victorian ideals of beauty - are actually forgeries, fashioned and planted in situ by Evans' local Cretian workers. Hehe, crafty Imperial backlash! Nonetheless, this 'goddess' figure was definitely a prominent icon in Minoan and later Mycenaean iconography. Minoan Crete was in fact administered through a chieftain governmental structure and at its apex were powerful priestesses holding term in the temple institutions. I in fact believe these images of 'goddesses' - statues, figurines, depictions on stamp seals etc - to be actualised representations of priestesses: powerful women holding religio-political roles in Bronze Age Minoan society. That we attribute a solely 'Goddess status' to any representation of a woman in Minoan - and by extension any prehistoric societies - denies the power and agency of real women acting in prehistory.
Lastly, I might add that evidence of opioid use is found ubiquitously in the archaeology: seeds and implements in the material culture etc. Many of these 'goddess' idols hold poppies and pipes. The 'upraised arm' pose demonstrated by many of the women in the iconography was most plausibly used for the purposes of conveying an ecstatic altered state of consciousness. If you ever get a chance to look at some of the stamp seals, you'll see what i mean (people lying about hallucinating in total reverie ;) ).
Fast Track Digestion may be of interest for those with SIBO. He has charts of the "fermentative potential" of various foods so that you can construct menus that work for you.
@ LifExtension,
I found the Goddess image after reading Electra by Henry Treece. He writes about the conflict between Minoan matriarchal and Achaean patriarchal religion and politics in early Greece in some pretty wonderful fictions, especially Electra.
She is the priestess, but the priestesses in Electra talk of the Goddess. Interesting story about the forgeries, and the Victorians were also obsessed with opium. The Minoan frescos are spectacular - and, they invented the flush toilet!
("She is the Goddess" being a quote from Electra)
Some more on SIBO: Chris Kresser's take
http://chriskresser.com/fodmaps-could-common-foods-be-harming-your-digestive-health
And Bill Lagakos's summary of how various diets work
http://caloriesproper.com/?p=3195
If you want more info, he has written a whole book on the subject, My Tummy Hurts.
http://tiny.cc/mytummyhurts
George you might find this interesting given the post. http://www.jackkruse.com/what-is-peripheral-neuropathy/
Very interesting Jack, good information on polyols.
I think what lipoic acid does is speed up the TCA cycle, it's the central rotor for the pyruvate>acetylCoA enzyme complexes, and supplying extra is a way of stoking more glucose into the mitochondria - and away from the polyol pathway.
Zinc and Mg are NMDA receptor ligands, and NMDA is the receptor implicated in withdrawal symptoms of opioids, alcohol, cocaine.
"Zinc and magnesium are potent inhibitors of the NMDA receptor complex"
http://www.ncbi.nlm.nih.gov/pubmed/11985339
FOOD GROUP TO SPLIT - IRRECONCILABLE DIFFERENCES CITED" is a headline I expect to see any day now. The notion of the Food Group seems to have become the most abused concept in Nutrition.
Aicar
CJC 1295 with DAC
Thanks for sharing this post! I like your post....
Pinnacle Peptides
Appreciate it intended for this fascinating document the following. My partner and i ended up being in search of similar to of which pertaining to a reasonable time and also at long last I've found the item the following. Pinnacle Peptides
Post a Comment