This little paper should have made a minor splash in the paleosphere last week, but no-one really knew what to do with it.
It has 20 authors. Success has a thousand fathers, they say.
Endogenous fructose production and metabolism in the liver contributes to the development of metabolic syndrome
Abstract
Carbohydrates with high glycaemic index are proposed to promote the development of obesity, insulin resistance and fatty liver, but the mechanism by which this occurs remains unknown. High serum glucose concentrations are known to induce the polyol pathway and increase fructose generation in the liver. Here we show that this hepatic, endogenously produced fructose causes systemic metabolic changes. We demonstrate that mice unable to metabolize fructose are protected from an increase in energy intake and body weight, visceral obesity, fatty liver, elevated insulin levels and hyperleptinaemia after exposure to 10% glucose for 14 weeks. In normal mice, glucose consumption is accompanied by aldose reductase and polyol pathway activation in steatotic areas. In this regard, we show that aldose reductase-deficient mice are protected against glucose-induced fatty liver. We conclude that endogenous fructose generation and metabolism in the liver represents an important mechanism by which glucose promotes the development of metabolic syndrome.
Carbohydrates with high glycaemic index are proposed to promote the development of obesity, insulin resistance and fatty liver, but the mechanism by which this occurs remains unknown. High serum glucose concentrations are known to induce the polyol pathway and increase fructose generation in the liver. Here we show that this hepatic, endogenously produced fructose causes systemic metabolic changes. We demonstrate that mice unable to metabolize fructose are protected from an increase in energy intake and body weight, visceral obesity, fatty liver, elevated insulin levels and hyperleptinaemia after exposure to 10% glucose for 14 weeks. In normal mice, glucose consumption is accompanied by aldose reductase and polyol pathway activation in steatotic areas. In this regard, we show that aldose reductase-deficient mice are protected against glucose-induced fatty liver. We conclude that endogenous fructose generation and metabolism in the liver represents an important mechanism by which glucose promotes the development of metabolic syndrome.
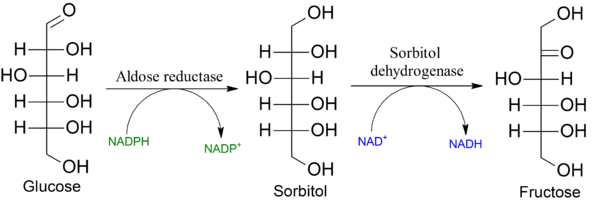 |
| The Polyol Pathway |
To summarise - when extra glucose is consumed by mice, some of this is converted to sorbitol then to fructose. This is associated with elevation of AST and ALT. Mice that cannot convert convert glucose to sorbitol are protected from rises in fructose and liver enzymes. Therefore fructose is so bad for you that it even accounts for the metabolic harm of high glucose intakes.
"These studies show that glucose-mediated obesity, visceral fat accumulation, hyperinsulinaemia, hyperleptinaemia and fatty liver are all dependent in part on the conversion of glucose to fructose in the liver with the metabolism of fructose by KHK. In other words, the mechanism by which glucose induces its metabolic effects is largely dependent on fructose
metabolites resulting from the fructose generated from glucose by the polyol pathway".
But, one must insist - this is dietary glucose doing this, not dietary fructose. This is not evidence in support of the idea that fructose is the bad carb, and glucose is the good carb; it looks more like evidence that, in normal metabolisms, sugars are somewhat interchangeable.
If you consume an excess of glucose, hepatic metabolism will have to convert some of that excess to fatty acids. Palmitic acid will be synthesised, and some palmitic acid will be elongated to oleic acid (because you can't make a triglyceride with 3 SFAs - if there's no dietary MUFA, DNL oleate makes the process of esterification possible). But you'll also need glycerol, and fructose is said to be a better glycerol substrate than glucose (for some reason I don't understand, being hopeless at maths). Note the pyruvate as a source of fatty acids in the schema below - this could just as easily have come from glucose. Indeed, the acetyl-CoA to make fatty acids could have come from fatty acids. (This is what happens with linoleic acid in fatty liver disease. Indeed, this kind of futile cycling of lipid carbons seems to be a feature of NAFLD.)

In the context of hyperglycemia in the absence of dietary fructose, (one might speculate that) the generation of a little fructose makes sense, just as the elongation of palmitate to oleate makes sense, as a means of packing away energy from glucose into stable triglycerides (which can be exported from hepatocytes with VLDL, or stored more-or-less safely for a while) more easily than would otherwise be the case. Perhaps.
 |
| We fed the mice 10% glucose water and off they went. |
The knock-out mice that couldn't change glucose into fructose consumed less glucose. The authors pulled out some KO mice (n=4) that ate as much as 4 non-KO mice, to show that the KO mice were healthier - fully protected against the metabolic harm of fructose/glucose - but this kind of post-hoc tactic is a bit suspect. Interestingly the KO mice had higher serum beta-hydroxybutyrate (ketone body) levels. I guess that energy had to go somewhere (is this at all relevant to the claims that potatoes elevate ketones?).
There are humans who cannot metabolise fructose or sorbitol.
"Affected individuals are asymptomatic and healthy, provided they do not ingest foods containing fructose or any of its common precursors, sucrose and sorbitol. Most adult patients do not have any dental caries".
Bill Lagakos says that his nutrition tutors spent all of five minutes on the polyol pathway; R.D. Feinman, who should know, states "I never saw the point or function of the polyol pathway".
Wild speculation aside, that's fair comment. The polyol pathway is useful for blinding diabetics, but it doesn't seem particularly essential for life. At most it might once have provided a slight buffer against hyperglycemia, but today we have far too many copies of the amylase gene and the polyol shock absorber, if that is what it was, is easily broken, making things worse. Is that any explanation? Some mysteries, it seems, are going to remain mysteries.
Fructose is a factor in fibrosis of chronic Hepatitis C: but it's not a biggie.
Industrial, not fruit fructose intake is associated with the severity of liver fibrosis in genotype 1 chronic hepatitis C patients.
Unhealthy food intake, specifically fructose, has been associated with metabolic alterations and with the severity of liver fibrosis in patients with non-alcoholic fatty liver disease. In a cohort of patients with genotype 1 chronic hepatitis C (G1 CHC), we tested the association of fructose intake with the severity of liver histology.
METHODS:
Anthropometric and metabolic factors, including waist circumference (WC), waist-to-hip ratio (WHR), dorso-cervical lipohypertrophy and HOMA were assessed in 147 consecutive biopsy-proven G1 CHC patients. Food intake, namely industrial and fruit fructose, was investigated by a three-day structured interview and a computed database. All biopsies were scored by an experienced pathologist for staging and grading (Scheuer classification), and graded for steatosis, which was considered moderate-severe if ⩾20%. Features of non-alcoholic steatohepatitis (NASH) in CHC were also assessed (Bedossa classification).
RESULTS:
Mean daily intake of total, industrial and fruit fructose was 18.0±8.7g, 6.0±4.7g, and 11.9±7.2g, respectively. Intake of industrial, not fruit fructose, was independently associated with higher WHR (p=0.02) and hypercaloric diet (p=0.001). CHC patients with severe liver fibrosis (⩾F3) reported a significantly higher intake of total (20.8±10.2 vs. 17.2±8.1g/day; p=0.04) and industrial fructose (7.8±6.0 vs. 5.5±4.2; p=0.01), not fruit fructose (12.9±8.0 vs. 11.6±7.0; p=0.34). Multivariate logistic regression analysis showed that older age (OR 1.048, 95% CI 1.004-1.094, p=0.03), severe necroinflammatory activity (OR 3.325, 95% CI 1.347-8.209, p=0.009), moderate-severe steatosis (OR 2.421, 95% CI 1.017-6.415, p=0.04), and industrial fructose intake (OR 1.147, 95% CI 1.047-1.257, p=0.003) were independently linked to severe fibrosis. No association was found between fructose intake and liver necroinflammatory activity, steatosis, and the features of NASH.
CONCLUSIONS:
The daily intake of industrial, not fruit fructose is a risk factor for metabolic alterations and the severity of liver fibrosis in patients with G1 CHC.
Excuse me, but OR 1.147 is not a huge correlation. It's as tiny as a red-meat-and-disease-of-your-choice correlation in a study run by vegans. What if they had looked at total carbohydrate? Or included fruit juice and high-GI glucose sources like bread and pasta? Do you think the OR would have been higher then? It was about OR 2.9 for carbohydrate and fibrosis in the last Italian diet study I read.
If we can learn anything from the polyol pathway, it is, that carbs will be carbs.
12 comments:
Sorbitol was part of the triumvirate put forth by Michael Brownlee in his Grand Unified Theory of Diabetic Complications.
The missing link: a single unifying mechanism for diabetic complications.
http://www.ncbi.nlm.nih.gov/pubmed/10997687
a bit overly simplistic, but it all *makes sense.*
That looks good; the induction of aldose reductase also promoting cholesterol accumulation via taurine depletion, being another possible mechanism increasing ROS.
I have this vision of the PP as a kind of glycemic shock absorber, that can send extra glucose to fructose and back, delaying its metabolism.
But depleting NADPH will deplete reduced glutathione, and NADH will add to reductive stress, when there is too much glucose.
(Wow, it seems some of those guesses were correct: I must actually be learning something here)
AR reduction of glucose to sorbitol probably contributes to oxidative stress by depleting its cofactor NADPH, which is also required for the regeneration of GSH. Sorbitol dehydrogenase, the second enzyme in the polyol pathway that converts sorbitol to fructose, also contributes to oxidative stress, most likely because depletion of its cofactor NAD+ leads to more glucose being channeled through the polyol pathway. Despite a more than 100% increase of MDA, oxidative stress plays only a minor role in the development of cataract in this acute diabetic cataract model. However, chronic oxidative stress generated by the polyol pathway is likely to be an important contributing factor in the slow-developing diabetic cataract as well as in the development of other diabetic complications.—Lee, A. Y. W., Chung, S. S. M. Contributions of polyol pathway to oxidative stress in diabetic cataract
http://www.fasebj.org/content/13/1/23.full
BRILLIANT, George.
Here we go - at last a paper that shows that the polyol pathway is useful in the kidney even if it supplies no answers as to why.
Aldose Reductase-Deficient Mice Develop Nephrogenic Diabetes Insipidus
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC86061/
We developed mice deficient in this enzyme and found that they had no apparent developmental or reproductive abnormality except that they drank and urinated significantly more than their wild-type littermates. These ALR2-deficient mice exhibited a partially defective urine-concentrating ability, having a phenotype resembling that of nephrogenic diabetes insipidus.
Maybe ARKO mice are also short-sighted, but no-one has taken them to the optometrist just yet.
Always enjoy your posts, George, just don't know enough to provide constructive comments. Instead, and because I don't have a blog, I post irrelevant papers that make me laugh. Sorry 'bout that - http://www.nutritionandmetabolism.com/content/10/1/58
"When people move towards a low-fat, plant-based diet, HDL levels decrease while other indicators of cardiovascular risk improve. This observation raises questions regarding the value of using HDL levels as a predictor of cardiovascular risk in populations who do not consume a typical western diet."
Of course raising questions regarding the use of LDL levels in populations who do not consume a typical low fat diet would be preposterous.
Ooh, you're gonna hate me - http://www.nutritionandmetabolism.com/content/10/1/59
"Results suggest that circulating low TC levels are associated with higher oxidative DNA damage."
I don't know what 8-hydroxydeoxyguanosine is, but it sounds bad.
Yup, it's bad. If you worked at Fukushima, you'd want to get your TC up. Difference in peroxidation rates of SFAs (if they elevate TC) and PUFAs (if they lower it) could account for some of this correlation.
A little bit of fructose helps the glucose go down (even without polyols)
http://www.ncbi.nlm.nih.gov/pubmed/12806219
Catalytic quantities of fructose (<10% of total carbohydrate flux) enhance liver glucose uptake in a dose dependent manner. The primary fate of the glucose is glycogen synthesis. The ability of fructose to augment liver glucose uptake is not impaired by the presence of marked insulin resistance such as in type 2 diabetes or infection.
George, any clue how relevant glucose conversion to fructose is in human metabolism? this can be huge pinning carbohydrate as a truly pathogenic, obesigenic, macronutrient more than we appreciated.
I think it shows that anyone demonizing fructose has to consider that glucose is just not so different. Conversion of fructose to glucose is a much bigger pathway than glucose to fructose, sugar is only half fructose, yet they'll still say only fructose is bad.
Whereas I would tend to go with GI, or rather rate and amount of serum carbohydrate availability whether F or G, as long as glucose/fructose stays in normal range after eating I wouldn't expect healthy person to be harmed, but that would eating smaller amounts of carbohydrate and more fat, protein, fibre, vinegar than is usual today.
But once someone has elevated fasting BG? That means they are well adapted to go without most dietary carbohydrate and will enter ketosis relatively easily.
Diabetes means someone has started carb restriction metabolism involuntarily while still consuming carbs. Keeping on eating more carbs will flood the engine.
It is not a big conversion and probably equals at most the <10% catalytic amount of fructose (not that I know, but that would be an adaptive amount).
The polyol pathway is one of those pathways that can accumulate toxic levels of intermediates (sorbitol), though probably not in liver which can dispose of fructose; it's part of what makes high glucose levels destructive.
Post a Comment